|
Q:
What is Interventional Cardiology?
A: Interventional Cardiology has emerged more
than a decade ago as an alternative to traditional
cardiac surgery. Through the use of minimally invasive
catherter-based techniques and innovative drug therapies
and devices, many conditions can now be treated without
surgery or lengthy hospital stays.
[back
to the top]
Q: What are Interventional Procedures?
A: Depending on the patient's specific condition,
an inteventional procedure can involve several techniques
and devices including the following:
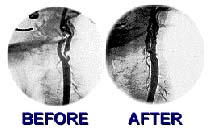
Angioplasty - a 40-minute procedure in which
a small balloon is inserted in an artery via a catheter
and inflated to open an area of blockage.
Atherectomy - a procedure involving a catheter
with a rotating tip that either breaks up calcified
plaque into very small particles or removes the plaque.
Stent - a small mesh sleeve, used over an angioplasty
balloon an left in place as a framework to keep an
area of blockage open. Recent developments of new
stents that are coated with drugs to help prevent
recurrence of blockage due to formation of scar tissue
(restenosis) are revolutionary techniques.
Radiation Therapy - also known as bracytherapy,
is used as an adjunct to other treatments to help
prevent restenosis or its recurrence following stent
implantation.
Drug therapies are also used to enhance the patient's
recovery and recuperation while minimizing the chance
of the condition's recurrence.
Recent advances in medical imaging, such as MRI (magnetic
resonance imaging) and IVIS (intravascualr ultrasound),
allow for highly precise views of the interior of
the heart and of the blood vessels.
[back
to the top]
Q: What is Coronary Artery Disease?
A: Coronary artery disease also known as atherosclerosis
is a disease of the heart arteries. This is a build
up of plaque or fatty deposits inside the artery.
This build up of plaque can block the flow of blood
to the heart causing chest pain, heart attack, or
other symptoms of heart disease. Coronary artery disease
can be reduced by changes in diet and lifestyle as
well as with some medications.
To diagnose coronary artery disease you may be asked
to undergo an angiography procedure (heart catheterization).
The angiography is done in the catheterization laboratory
at the hospital. During this procedure the patient
is sedated and a small sheath (short hollow tube)
is inserted through a puncture site in the groin area
(femoral artery). Through this sheath a catheter is
maneuvered to the heart arteries where a special dye
is injected and x-ray pictures can be taken of the
heart arteries. If treatment is needed, the interventional
or non-surgical procedures can be done through this
sheath.
Treatment for coronary artery disease can be done
surgically by coronary artery bypass graft surgery
(CABGS) or non-surgically by percutaneous coronary
intervention (PCI). These non-surgical procedures,
which can be done in the catheterization laboratory,
are listed in Procedures.
[back
to the top]
Q: What is Peripheral Vascular
Disease?
A: Like the heart arteries plaque can build
up in any artery of the body. PVD is plaque build
up in the arteries supplying blood to the arms, leg
and brain. Risk factors that contribute to PVD are
smoking, high blood pressure, family history, high
cholesterol, and diabetes. Symptoms of PVD to the
legs are claudication (pain in the legs especially
when walking that is relieved when resting), numbness
or tingling in the legs or feet, coldness in the legs
or feet, and/or ulcers of the legs or feet that do
not heal. The non-surgical treatment for peripheral
vascular disease is balloon angioplasty and stenting.
[back
to the top]
Q. What do I do before a scheduled
procedure?
A: Review the Pre-Procedural
Information. If you need further clarification,
or if any of the information is unclear, contact us
or your doctor before the scheduled procedure is to
take place.
[back
to the top]
Q: What are the "do's and dont's"
after a procedure?
A: Review the Post-Procedural
Information. If you need further clarification,
or if any of the information is unclear, contact us
or your doctor before the scheduled procedure is to
take place.
[back
to the top]
Q: What are Drug Coated Stents?
A: Drug coated stents, also called medicated
stents can be used to treat Coronary Artery Blockages.
These stents are coated with a time-released medication
which can prevent the occurance of restenosis (development
of scar tissue that re-blocks the artery at the original
site. These medicated stents are particularly useful
for small to medium size arteries. In larger arteries,
a non-medicated stent is as beneficial as a medicated
stent.
[back
to the top]
Q: Are there any special precautions
with medicated stents?
A: Yes. There is a higher risk for a clot formation
following the implantation of these stents. Drugs
such as Plavix (along with aspirin) can reduce the
risk of complications. These drugs are to be continued
for at least 4 to 6 months. DO NOT STOP TAKING THESE
MEDICATIONS, unless directed by your physician.
[back
to the top]
Q: What is High Risk Angioplasty
& Cardiopulmonary Support (CPS)?
A: High-risk angioplasty means angioplasty
in patients who have poor LV function alone or with
other medical conditions that make them a high risk
candidate for angioplasty or even bypass surgery.
We mean people who have had previous multiple myocardial
infarctions with multiple coronary stenoses. Or they
have only one open artery which is also threatening
to close. In these high risk patients, one cannot
perform angioplasty or any other intervention because
their heart will not tolerate the procedure. But with
the support of the Percutaneous Cardiopulmonary Bypass
Support (PCPS), the procedure can be performed very
safely, even in patients in ventricular fibrillation.
[back
to the top]
Q: What is Percutaneous Transmyocardial
Revascularization (PTMR)?
A: There are many patients who because of small
size vessels or diffuse disease are not good candidates
for percutaneous interventions or bypass surgery.
These patients become severely limited because of
incapacitating angina. Percutaneous Transluminal Myocardial
Revascularization (PTMR) can provide these with symptomatic
relief of angina. In some animals, like crocodiles
and alligators, the blood flow to the heart muscle
is directly from the LV chamber via small channels.
Based on this knowledge, Dr. Mirhoseini created channels
in human hearts using laser energy. Over the last
few years other surgeons have created similar laser
channels directly into the heart muscle with objectively
evident beneficial effects. However, the surgical
method is more invasive and is associated with 10-19%
mortality. Now, using catheter-based technology, Dr.
Shawl is able to create channels from inside the chamber
of the human heart into the LV muscles and performed
the first few cases in India without any complications.
Today, Dr. Shawl and his team performs PTMR in the
U.S. with FDA IDE approval and has performed a number
of cases with great success and promising results.
Dr. Shawl also presented the results of these early
experiences at the ACC meeting in Atlanta. At six
months, 9 out of 12 patients showed objective improvement.
[back
to the top]
Q: What is Carotid Stenting?
A: Carotid Stenting basically involves the
same technique as for coronary angioplasty. Initially,
we dilate the lesion with balloon angioplasty and
then place a stent across the blockage. The whole
procedure takes only half an hour to 45 minutes and
the risks are considerably less than carotid surgery,
even though carotid stenting is just evolving. Further
refinement in equipment and technique greatly reduces
the risks. Carotid artery stenting is done to prevent
future strokes in people with a blockage in the carotid
artery. See New Stroke Treatment to learn more.
[back
to the top]
Q: What is Hybrid MIDCAB/PTCA?
A: This is an "integrated minimally invasive
approach" or "hybrid procedure". The only advantage
of conventional bypass surgery is excellent outcome
with arterial conduits like LIMA, RIMA, radial or
gastroepiploic vessels. Dr. Shawl uses these conduits
by minimally invasive (MIDCAB) surgery. In patients
with multiple vessel disease, instead of conventional
CABG, Dr. Shawl combines the use of MIDCAB and percutaneous
intervention.
In the last 30 cases+ at Washington Adventist Hospital,
Dr. Shawl and his team have performed MIDCAB initially
and then percutaneous interventions to the remaining
vessel the next day. In the new operating room and
cath lab, the MIDCAB and percutaneous interventions
can be performed at the same sitting. This is revolutionary
and the leading model for bypass and interventions
in which occur at the same place and the same day.
There are also new introductions of Robotic Technology.
This method uses robotic arms that are inserted into
the chest in four small holes about the size of a
pencil. The surgeon "operates" from a comfortable
console about ten feet away from the patient by viewing
a 3-D image of the operational field through a tiny
camera in the patients body. This new technology allows
the surgeon to perform minimally invasive surgery
and angioplasty at the same time.
[back
to the top]
|